
Patterns in clinical practice don’t shift overnight. But when they do, they quietly demand our attention.
Something unusual has been happening at Physio Active India over the past couple of years. Frozen shoulder-scientifically known as adhesive capsulitis (inflammation that causes shoulder stiffness and pain)-is no longer showing up the way the textbooks said it would. The patient profile is changing, the triggers are evolving, and if we are still treating it like it is 2019, we are missing something critical.
The Patient Who Doesn’t Fit the Textbook
Picture this: A 37-year-old walks into our Gurgaon clinic. No history of diabetes. No thyroid issues. No physical trauma. Just a shoulder that has been progressively tightening up over the past few months, stealing their range of motion one degree at a time.
Ten years ago, this patient would have been an outlier. Today? They are becoming the norm.
The Old Checklist: Frozen shoulder used to come with predictable baggage-usually affecting individuals over the age of 50, or those managing metabolic conditions and prolonged immobilization.
But the shoulder pain clinic looks entirely different now. We are regularly seeing patients in their mid-30s and early 40s with no obvious explanation and no clear injury. Just pain that won’t quit and stiffness that creeps in, night after night.
What changed?
The Two Elephants in the Room
When we look closely at recent patient histories, two consistent patterns emerge that are simply too frequent to dismiss as coincidence.
1. Localized Inflammatory Triggers
Clinical honesty demands that we look at all localized triggers. A small but noticeable number of patients present with shoulder pain following routine deltoid injections – including vaccinations, which then progresses into adhesive capsulitis.
This isn’t about rhetoric; it’s about pure clinical observation. In certain susceptible individuals, a strong localized inflammatory response in the deltoid can act as the spark that ignites the broader frozen shoulder cascade. It is a physical trigger that deserves careful investigation, not dismissal.
2. The Post-Viral Inflammatory Shadow
Recovery from viral infections isn’t always a straight line. Often, a lingering inflammatory presence can haunt multiple body systems long after the initial sickness has passed.
We are seeing a distinct timeline: patients who recovered from viral infections six to twelve months prior are now presenting with frozen shoulders. With no other risk factors present, the inflammation works quietly behind the scenes, affecting connective tissue and triggering complex immune responses. Frozen shoulder has become the uninvited guest that shows up long after the initial illness has cleared.
The Treatment Mistake That Keeps Happening
Here is a truth we need to talk about openly: most patients experiencing shoulder pain don’t see an orthopedic surgeon first. They come to a physiotherapy clinic. This means physiotherapists aren’t just treating – we are diagnosing. We are the gatekeepers.
And here is where things frequently go wrong in early – stage care:
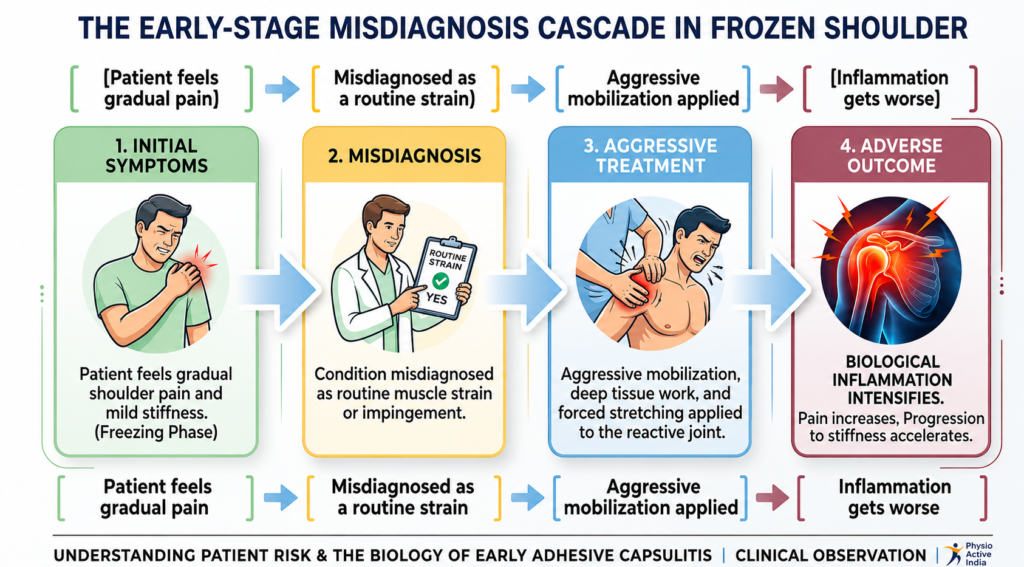
When a patient isn’t responding to a standard rotator cuff protocol, the temptation is to push harder, use deeper soft tissue work, or try to “break up the scar tissue.”
In the early stages, aggressive treatment is gasoline on a fire. The shoulder tissue is already highly reactive and angry. Forcing it into painful ranges escalates the pain, intensifies the biological inflammation, and actually accelerates the freezing process.
Why Timing Defines Recovery
Frozen shoulder is a moving target. It progresses through three distinct phases, and using the right technique at the wrong time can actively cause harm.
| Phase | What the Tissue is Doing | Correct Therapeutic Approach |
| 1. Freezing (The Pain Phase) | High inflammation, extreme night pain, hypersensitivity. | Gentle relief. Protect the joint, manage pain and avoid aggressive stretching. |
| 2. Frozen (The Stiffness Phase) | Pain begins to back off; severe loss of range of motion. | Controlled mobility. Gentle capsular stretching within pain tolerance. |
| 3. Thawing (The Recovery Phase) | Range naturally begins to return; tissue is less reactive. | Progressive loading. Aggressive rehab, strength building, and functional restoration. |
Aggressive mobilization during the Freezing phase causes damage. The exact same aggressive mobilization during the Thawing phase saves the shoulder. Timing is everything.
What Needs to Change Right Now
If the condition is evolving, our clinical intuition must evolve with it. We are focusing on four immediate shifts:
- Sharpen Clinical Suspicion: When a 35-year-old presents with gradual shoulder stiffness and a history of systemic inflammation, don’t automatically assume a simple impingement. Keep adhesive capsulitis on the radar.
- Respect the Flame: Stop pushing through sharp pain in early stages. Our role early on is to educate, provide pain relief and maintain gentle mobility without forcing ranges that aren’t ready to open.
- Build Better Medical Bridges: Physiotherapists and orthopedic specialists need to collaborate much earlier. Realizing when a patient needs a timely medical intervention-like a corticosteroid injection to calm phase-one inflammation-is a sign of smart, collaborative care.
- Speak with Warm Honesty: We need to give patients a realistic timeline. Frozen shoulder is a journey that often takes a year or more to fully resolve. Our job is to give them the patience, appropriate exercises, and emotional support to see it through.
The Bottom Line
The patients walking through our doors are younger, the triggers are more complex, and the presentations are shifting. Clinical practice cannot rely solely on old protocols; it requires us to actively watch the patterns happening right in front of us.
The condition is changing. As care providers, we have to change too.
This clinical perspective is inspired by the insights shared by Dr. Manoj DM on LinkedIn. For more detailed medical discussions, you can view the original professional thread here.
Reach out to us to schedule a session:
WhatsApp / Call : 9971879090
Email: info@physioactiveindia.com
In case you need personal consultation, feel free to book a session with us today
Schedule the session from our website




{kind=link}
{kind=link}